
COVID-19: MORE MISUNDERSTANDINGS (Part 1/2): Vaccines Working? "Natural Immunity," Schools, Weed
- Dr. Bow Tie

- Jan 30, 2022
- 7 min read
Updated: Feb 1, 2022
As we hit the two-year anniversary of the pandemic hitting the United States, it's important to reflect on what we have learned. The most important lesson is that science evolves as we learn more, and sometimes things we hypothesize turn out to be wrong, and we must correct that. Another important lesson, though, is that we do understand certain principles that have held up over time, and we can base our scientific consensus on those principles. This is really vague, so let's get into some specifics. Let's answer some questions!
WHY ARE WE BOTHERING WITH VACCINES WHEN THEY DON'T WORK?
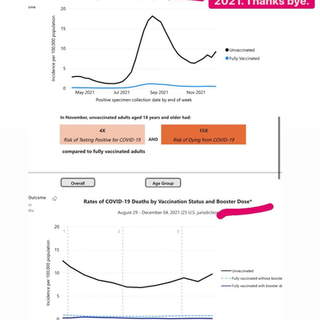
I'm seeing a few statuses lately of "Well, we know the vaccines don't work now, so why are we still pushing them?" Except that this is not true. The vaccines absolutely are working. If you break down deaths data (see below, h/t EpidemiologistKat), even state by state, the amount of people hospitalized (especially those in the ICU) who are unvaccinated far outnumber those who are vaccinated. This also applies to reinfections - people who are not fully vaccinated get reinfected far more often than those who are vaccinated. More on that below.
Yes, you can still catch COVID-19 even if you are vaccinated. No one ever said otherwise! That's why we should still be utilizing mitigation measures such as masking and distance. The main measure of vaccine efficacy has always been prevention of severe illness/hospitalization/death, and they do that in spades*!
*At this point, full vaccination includes a booster/third dose. This is not the first vaccine to require boosters - most of us have had multiple doses of a vaccine to maintain immunity (meningitis, HPV, MMR, Tdap). We have seen that Omicron seems to evade two doses due to immunity waning over time (on the graphs below, you see death rates among “fully vaccinated” start to rise at the end of December because that category is still mostly not boosted), but three doses still helps you fight it. And we ARE seeing that, even though it wasn't the main measure, that vaccines do prevent infections and transmission WHEN they are widespread in an area (vaccines are a collective health measure).
Someone recently responded to me with "You can show whatever data or papers you want, I'll believe what I see with my own eyes." Science and the scientific method only start with anecdotal observations, though. From there you form a hypothesis and then that hypothesis must undergo experimentation with multiple trials and be applied across a larger population. When possible, larger and well-conducted trials (like we had for vaccines, boosters, vaccines for kids) or at least larger real-world observations are better evidence.
WHY ARE YOU IGNORING "NATURAL IMMUNITY"?
WAIT, WHY ARE YOU CALLING THAT A MISNOMER?
Anti-vaccination campaigns have loved to try to mislabel vaccine effects (and the vaccines themselves). First of all, yes, the mRNA vaccines ARE vaccines, and anyone who tells you otherwise does not have a sufficient understanding of what vaccines are.
The idea of "natural immunity" as it's widely used is a misrepresentation. Immunity from vaccines is still natural, because it's still YOUR immune system. The discussion should be how infection-mediated immunity fits with vaccine-mediated immunity. Since the vaccines emerged, people have tried to discuss infection-mediated immunity as equal or superior to vaccine-mediated immunity, a reason not to have to get vaccinated. I have cited data multiple times about how infection-mediated immunity is real, BUT both less reliable and less permanent. People have told me that they have gotten their antibodies checked (not the most accurate measure anyway) and they're no longer present >3 months after infection, but despite that acknowledgement, they still refuse to believe the data in favor of vaccination.
Most recently, the CDC put out a new MMWR based on data gathered during the Delta peak (so pre-boosters and pre-Omicron). It showed that rates of hospitalizations/ED visits decreased the most among those who had a combination of vaccine-mediated+infection-mediated immunity (mostly got vaccinated after having a previous COVID infection). This was followed by the decrease in those who had infection-mediated immunity only, vaccine-mediated immunity, and then no immunity.
A few things with this:
Maybe this could have made a case for infection-mediated immunity requiring no vaccine (against Delta; not as applicable to previous variants), except that we already knew that two doses did have some wane of immunity over time, which is why we had already started talking about boosters.
The number of previous-COVID-without-vaccine is somewhat low in the paper, and they don't stratify by severity of previous infection, so we don't know how many people had mild infections and then developed longer-lasting antibodies (less likely) and how many people had to come back from death's door (and maybe are still recovering so they don't socialize as much, meaning less exposure).
People who have recovered from previous COVID without full vaccination (3 doses of mRNA) are 5x more likely to be reinfected with Omicron, meaning the findings of the MMWR are no longer as relevant.
Getting COVID to develop immunity to COVID (or thinking that previous infection-mediated immunity is enough now) is not a wise strategy. You are not guaranteed a mild infection just because you're "young and healthy" (try telling that to the previously-healthy folks in our hospitals and ICUs). Further, even a mild, non-hospitalized COVID-19 infection can lead to PAS-C ("long COVID"), resulting in everything from months-long loss of smell/taste (or abnormal smell/taste, which can be even worse) to oxygen requirements to chronic severe fatigue to many other issues.
WHY ARE THEY TRYING TO FORCE MASKS AND VACCINES IN SCHOOLS? DOESN'T COVID SPARE KIDS?
WHY ARE WE HINDERING SOCIAL INTERACTION?
Once again, vaccine requirements and mask mandates in schools are hotly contested in the news and in school board meetings. People keep spouting the myth that "COVID doesn't affect kids" and that the "trauma" of masks is a terrible cost to our children's lives. Now, no one WANTS schools closed or forced home schooling, but the fact is, at this point of the pandemic, that Omicron affects children more.
A group of doctors just released the "Urgency of Normal" toolkit, pushing reopening of schools and dropping of mask mandates, subscribing to the falsehood that living with COVID means letting it rip and dropping all mitigation.
It's a lot of bullshit.
They misrepresent most of their data. They make certain claims (like saying pediatric suicide rates are increased) that are completely false, and the data they present actually proves them wrong (pediatric suicide rates are down the past two years - they had to go back and edit their slide). They blame school closures for children's mental health issues while not taking into the fact that the pandemic itself (including the loss of loved ones) playing a major role.
You know what the actual resilience of kids is? Kids can adapt to wearing masks just like adults do, as long as they have good role models. And no, it does not "hinder social interaction." The AAP has released research showing that children can learn social interactions and seeing the top halves of faces, even with masks...because for the most part those kids are not wearing masks at home and their parents' faces actually help with those cues.
At the end of 2021, over 1000 children had died from COVID and >6000 were suffering MIS-C (multi-system inflammatory syndrome due to COVID-19). There are also a great many suffering PAS-C ("long COVID") even without hospitalization. Since then, we have seen an average of 800 pediatric COVID hospitalizations EVERY DAY - not all end in death, but it is certainly disruptive to their education.
The Urgency of Normal authors also compare influenza to COVID-19, which we have already discussed as not comparable. However, if you want to try to compare them, deaths by the flu are down by record numbers. We have had more COVID-19 pediatric deaths in ONE WEEK than we had influenza deaths for the last two seasons (2020-21: 1 flu death, 2021-22: 5 flu deaths so far because less mitigation measures are in place; meanwhile, 27 kids died of COVID between 1/13-1/20, and it likely would have been worse without masking and vaccinations where able). And if your first response is "well, there will always be some deaths" you can shut up because children are not supposed to die, especially of a preventable illness.
Remember, a key reason for masking in schools is, similar to most workplaces, many schools cannot afford the ventilation or spacing needed to cut down spread, and especially at young ages, not enough kids are or are able to be vaccinated (even among those that could be now). Any potential risk of masking or school closures disrupting education (the latter is not without consequences, certainly) is far outweighed by the risk of spreading COVID to families (remember, >160,000 kids lost a caregiver this pandemic) or kids getting sick and/or dying from COVID themselves.
Meanwhile, a study from 2020 actually found that good masking actually reduced closures (Link below)! Combined with other mitigation measures, that can be utilized today.
Dr. Jonathan Howard states it best: "Schools are having trouble staying open because teachers and students are getting sick, not because politicians are closing them." It is COVID-19 that is disrupting society, not the mitigation measures meant to stop it.
Below is a link to Dr. Tyler Black's excellent thread debunking the "Urgency to Normal" toolkit.
SPEAKING OF KIDS, I STILL WORRY - IS THE VACCINE GOING TO AFFECT MY FERTILITY?
Thankfully, we have proven time and time again that the COVID-19 vaccines have no effect on pregnancy or fertility outcomes. Yet another paper just came out regarding this (applied to a population utilizing in vitro fertilization - link below). Across multiple populations and papers, we have studied patients with and without vaccines and looked at menstrual cycles, miscarriages/spontaneous abortions, birth defects, and premature births, and there were no differences in any of the pregnancy outcomes. Menstrual cycles may be thrown off for 2-3 cycles, but that is rare and, more importantly, temporary.
What is more likely to prevent menstrual cycles permanently? What is more likely to cause adverse pregnancy outcomes? COVID-19 infection. Get vaccinated and take steps to protect yourself and anyone who may be pregnant around you.
CAN SMOKING WEED PREVENT/TREAT COVID-19?
Nope.
In an in vitro study (remember, that’s just in test tubes/petri dishes, not actual humans), it was found that cannabigierolic acid (CBGA) and cannabidiolic acid (CBDA) had some effect against alpha and beta variants. It also required incredibly high concentrations to do so. So this is not yet applicable to humans, AND it was only seen against older variants so far (neither of which are currently dominant), AND to do so required an amount unreasonable for human consumption. Further, CBGA and CBDA are only found in fresh, uncured cannabis flowers (I am not a cannabis expert in any way, so I had to look some things up here). Drying and smoking cannabis causes a chemical reaction (decarboxylation) that converts the compounds to CBG and CBD, which are not shown to have effect against COVID. Believe me, I would love to tell you to use weed to prevent/treat COVID. It is not going to help you there.
Part 2 coming soon!
Urgency of Normal Debunk: https://twitter.com/tylerblack32/status/1486111652076527623





Comments